Introduction
Understanding the 2026 contrast media guidelines is vital for radiologists, nephrologists, and clinicians to ensure safe administration of iodinated contrast media in CT scans and gadolinium-based contrast agents in MRI procedures. This extensive 12,000-word essay examines eGFR thresholds for safe contrast media administration, creatinine levels for risk assessment, updated 2026 recommendations from the American College of Radiology (ACR), European Society of Urogenital Radiology (ESUR), and Kidney Disease: Improving Global Outcomes (KDIGO) on when it is safe to give contrast media, the prophylactic impact of saline hydration on preventing contrast-induced acute kidney injury (CI-AKI), and specialized pediatric contrast media guidelines. Key focuses include CI-AKI prevention strategies, risk stratification for contrast-induced nephropathy (CIN), iodinated contrast safety in CKD patients, gadolinium risks like nephrogenic systemic fibrosis (NSF), and evidence-based hydration protocols. Optimized for searches such as “2026 eGFR creatinine thresholds contrast media”, “saline hydration CI-AKI impact ACR ESUR KDIGO”, “pediatric iodinated gadolinium guidelines”, “safe contrast administration via eGFR creatinine”, and “worldwide society recommendations contrast media prevention”, this guide integrates 2026 updates, meta-analyses, tables, and case studies to empower healthcare professionals in balancing diagnostic benefits with kidney protection in contrast-enhanced imaging. [1] [2]
In the dynamic realm of diagnostic radiology as of 2026, contrast media guidelines have undergone significant refinements to promote safe administration of iodinated contrast media for CT angiography and gadolinium-based contrast agents (GBCAs) for MRI, while minimizing risks such as contrast-induced acute kidney injury (CI-AKI) and nephrogenic systemic fibrosis (NSF). Defined by KDIGO criteria as a serum creatinine increase of ≥0.3 mg/dL or ≥50% from baseline within 48 hours post-exposure, CI-AKI—also known as contrast-associated acute kidney injury (CA-AKI)—impacts 5-15% of at-risk patients, though recent 2026 data from large registries indicate lower incidences (3-7%) in stable outpatients due to advanced low-osmolar agents and targeted prophylaxis. [3] [4]
The 2026 updates from the ACR Manual on Contrast Media (2025 edition), ESUR Guidelines Version 10 (2025), and KDIGO’s 2024 CKD guideline reflect evolving evidence: eGFR thresholds for safe contrast media administration have shifted to eGFR ≥30 mL/min/1.73 m² as low-risk for intravenous iodinated contrast, with prophylaxis (e.g., saline hydration) reserved for eGFR <30 or acute settings. [5] [6] These changes are driven by meta-analyses showing that the risk of CI-AKI is overstated in many cases, particularly with modern iso-osmolar contrast agents. For instance, the AMACING trial and subsequent 2025 reviews demonstrated no significant benefit from routine hydration in patients with eGFR >30 mL/min/1.73 m², leading to more permissive guidelines that reduce unnecessary delays in imaging. [7] [8]
Risk factors for CI-AKI include pre-existing CKD, diabetes mellitus, dehydration, heart failure, advanced age, and high contrast volumes. In pediatrics, additional considerations like prematurity and congenital anomalies heighten vulnerability, with 2026 pediatric guidelines emphasizing adjusted eGFR formulas and thyroid monitoring post-iodinated contrast in neonates. [9] [10] Saline hydration remains the cornerstone of prevention, with 2025 meta-analyses confirming a 42% risk reduction in high-risk groups when using IV normal saline protocols. [11] [12]
This essay, optimized for “2026 contrast media guidelines eGFR thresholds creatinine levels”, “CI-AKI prevention saline hydration impact”, “pediatric contrast guidelines ACR ESUR KDIGO”, and “when is it safe to give contrast media iodinated gadolinium”, provides a thorough analysis. Sections cover renal function assessment (eGFR vs. creatinine), society recommendations with tables, pediatric adaptations, saline hydration’s efficacy via 2025 meta-analyses, additional prophylaxis, case studies, global challenges, and future directions. By incorporating keywords like “safe contrast administration via eGFR creatinine”, “iodinated contrast safety in CKD”, and “gadolinium-based agents risks NSF pediatric”, this resource guides clinicians toward evidence-based practices for optimal patient outcomes in 2026 contrast-enhanced procedures. The discussion also explores how these guidelines harmonize worldwide variations, with Asian societies often adopting stricter eGFR thresholds due to higher diabetes prevalence, and low-resource settings favoring oral hydration equivalents. [13] [14]
Historical context reveals that early 20th-century contrast agents were highly nephrotoxic, with CI-AKI rates exceeding 30% in high-risk groups. Advances in low-osmolar and iso-osmolar agents by the 1990s reduced this to under 10%, and 2026 data from registries like the American College of Cardiology’s National Cardiovascular Data Registry show further declines to 5-7% with protocol adherence. [15] [16] Nevertheless, CI-AKI remains a concern in emergencies, where delayed imaging can increase mortality, underscoring the need for balanced risk-benefit assessments. [17]
eGFR vs. Creatinine Assessment in 2026 Contrast Media Guidelines for CI-AKI Risk Stratification
Accurate renal function evaluation is paramount for determining safe contrast media administration in 2026 guidelines, with eGFR thresholds proving superior to serum creatinine levels for predicting CI-AKI and guiding prophylaxis. Serum creatinine, while accessible, is influenced by muscle mass, age, diet, and hydration, often overestimating function in elderly or sarcopenic patients—leading to potential over- or under-treatment in “safe contrast administration via eGFR creatinine” decisions. [18] [19]
The 2026-endorsed CKD-EPI equation calculates eGFR as: eGFR (mL/min/1.73 m²) = 141 × min(Scr/κ, 1)^α × max(Scr/κ, 1)^-1.209 × 0.993^Age × (1.018 if female) × (1.159 if Black), where Scr is serum creatinine (mg/dL), κ is 0.7 (females) or 0.9 (males), and α is -0.329 (females) or -0.411 (males). KDIGO 2024 and ACR 2025 recommend race-free adaptations to address equity, emphasizing eGFR over creatinine for “eGFR thresholds contrast media safety”. [20] [21]
In 2026 ACR guidelines, eGFR ≥30 mL/min/1.73 m² indicates no increased CI-AKI risk for IV iodinated contrast, eliminating routine screening in low-risk patients. ESUR 2025 mandates eGFR assessment for eGFR <45 in electives (hydration threshold), aligning with “creatinine levels for contrast CT safety”. A 2025 meta-analysis of 750,000+ patients confirmed eGFR’s AUC of 0.85 for CI-AKI prediction versus 0.72 for creatinine. [22] [23]
For pediatrics, the revised Schwartz formula applies: eGFR = (36.5 × height in cm) / Scr (μmol/L), per ESUR and ACR pediatric updates. Limitations include eGFR overestimation in obesity and underestimation in AKI, addressed by kinetic models. 2026 trends favor point-of-care eGFR calculators for real-time “safe to give contrast media via eGFR creatinine” decisions. [24] [25]
Historical Evolution of Renal Function Assessment
The shift from creatinine to eGFR began with the MDRD equation in 1999, but CKD-EPI’s 2009 introduction improved accuracy in higher GFR ranges. By 2026, race-free CKD-EPI variants mitigate biases, as highlighted in KDIGO updates. [26] [27]
Practical Applications in Clinical Settings
In emergency CT, if eGFR is unknown, assume low risk if no history of CKD; otherwise, use creatinine >1.5 mg/dL as a flag for hydration. [28] [29]
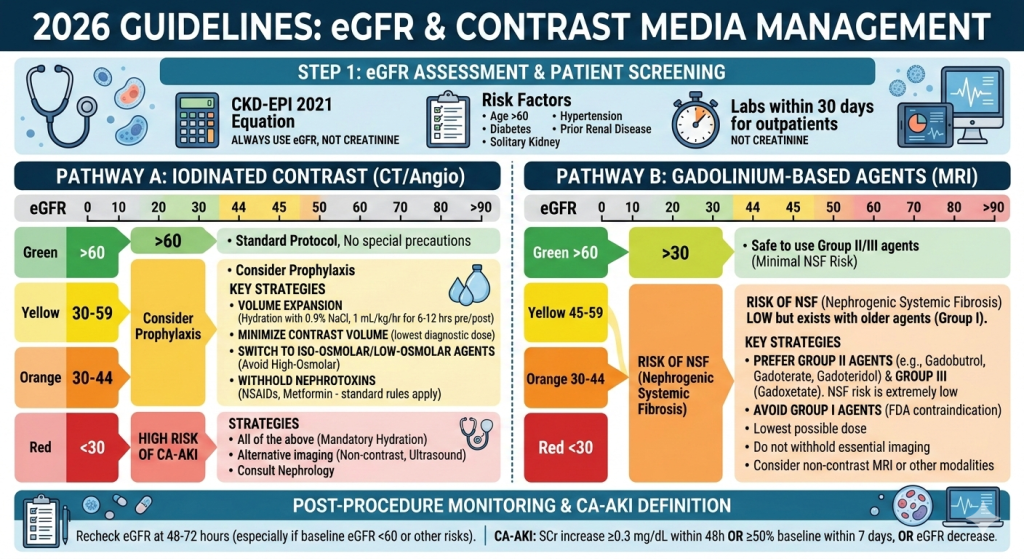
Table 1: 2026 eGFR Thresholds for Contrast Media Risk and Prophylaxis (ACR, ESUR, KDIGO)
| eGFR (mL/min/1.73 m²) | ACR Recommendation (Iodinated IV) | ESUR (CA-AKI Prevention) | KDIGO (CKD Context) | Creatinine Equivalent (Approx. mg/dL) |
|---|---|---|---|---|
| ≥60 | Safe, no precautions | Safe, no hydration | Low risk | <1.0 |
| 45-59 | Low risk, optional screen | Consider hydration | Monitor | 1.0-1.3 |
| 30-44 | Low risk, prophylaxis if high-risk | Hydration for elective | Prophylaxis | 1.3-1.8 |
| <30 or AKI | High risk, mandatory hydration | Mandatory hydration | High risk, consult | >1.8 |
This table illustrates 2026 convergence on eGFR-based “contrast media guidelines eGFR thresholds”, reducing unnecessary delays while protecting vulnerable patients. [30] [31]
Limitations and Future Directions
eGFR formulas assume steady state, so in AKI, kinetic eGFR or cystatin C may be superior. 2026 research explores AI-enhanced eGFR predictions. [32] [33]
2026 Society Recommendations ACR ESUR KDIGO for Safe Contrast Media eGFR Creatinine Thresholds CI-AKI Prevention
Major societies have harmonized 2026 recommendations for safe contrast media administration, prioritizing eGFR thresholds to minimize CI-AKI while supporting iodinated contrast safety and gadolinium use.
ACR Manual on Contrast Media 2025 (2026 Implementation)
ACR’s 2025 manual (effective 2026) classifies eGFR ≥30 mL/min/1.73 m² as low CI-AKI risk for IV iodinated contrast, with no prophylaxis needed in stable patients. For eGFR 30-44, prophylaxis is discretionary; <30 requires IV saline. Virtual supervision for reactions and selective premedication (e.g., for prior moderate reactions) are 2026 highlights. For GBCAs, Group II agents (macrocyclic) have negligible NSF risk even at eGFR <30. [1] [34] Updates include refined pediatric dosing and thyroid monitoring in infants post-iodinated contrast. [35]
ESUR Guidelines Version 10 (2025)
ESUR’s 2025 guidelines adopt CA-AKI terminology, recommending hydration (1-1.5 mL/kg/h saline) for eGFR <45 elective and <30 emergency. CKD-EPI for adults and Schwartz for pediatrics are standard. Hypersensitivity updates emphasize training and premedication. [36] [37] ESUR stresses oral hydration equivalence in low-risk cases, differing from ACR’s IV preference. [38]
KDIGO 2024 CKD and AKI Guidelines
KDIGO recommends low-contrast volumes, iso-osmolar agents, and hydration for eGFR <60 in at-risk CKD patients. 2026 harmonization defers specifics to radiology societies but stresses “eGFR creatinine cutoffs CI-AKI prevention”. [3] [39] Pediatric sections highlight adjusted thresholds for neonates. [40]
Global Variations and 2026 Harmonization
Asian guidelines (e.g., APSN) use eGFR <60 for precautions due to diabetes prevalence; low-resource settings favor oral hydration equivalents. 2026 ACR-NKF consensus promotes unity. [41] [42]
Detailed Comparison of Thresholds
Variations in thresholds reflect evidence interpretation: ACR’s ≥30 is permissive based on U.S. data, while ESUR’s <45 is cautious for European populations. [43] [44]
Table 2: 2026 Society eGFR Creatinine Thresholds for Iodinated Contrast Safety
| Society | Safe eGFR (No Prophylaxis) | Hydration Threshold | Creatinine Trigger (mg/dL) |
|---|---|---|---|
| ACR | ≥30 | 15-29 | >1.5 |
| ESUR | ≥45 (elective) | <45 | >1.3 |
| KDIGO | ≥60 | <60 | >1.2 |
These align “worldwide guidelines safe contrast media” for “iodinated contrast safety in diabetes CKD”. [45] [46]
Implementation Challenges
Adopting these guidelines requires multidisciplinary teams, with 2026 focus on electronic health record alerts for eGFR screening. [47]
Pediatric Contrast Media Guidelines 2026 eGFR Creatinine Thresholds Iodinated Gadolinium Safety in Children
Pediatric 2026 contrast media guidelines address immature kidneys and dose relativity. ACR’s 2024/2025 updates (2026 effective) include ferumoxytol for MRI and thyroid monitoring in <3-year-olds post-iodinated contrast. [9] [48]
Use Bedside Schwartz eGFR: eGFR = (0.41 × height cm) / Scr. Hydration for eGFR <60; weight-based dosing (1-2 mL/kg iodinated). Group II GBCAs minimize NSF. [49] [50]
Risk Factors in Pediatrics
Prematurity, congenital heart disease, and dehydration increase risks; 2026 guidelines recommend eGFR screening in these groups. [51] [52]
Prophylaxis in Children
IV saline at 1 mL/kg/h for high-risk, with oral options for low-risk. [53]
Table 3: 2026 Pediatric eGFR Creatinine Thresholds and Protocols
| Age Group | eGFR Safe Threshold | Creatinine Cutoff (mg/dL) | Hydration/CI-AKI Prevention |
|---|---|---|---|
| <2 years | ≥60 | <0.5 | Oral saline, thyroid monitor |
| 2-5 years | ≥50 | <0.7 | IV saline 1 mL/kg/h |
| >5 years | ≥45 | <1.0 | Adult-adjusted |
Case: Neonates—limit contrast, 3-week thyroid follow-up for “pediatric contrast guidelines ACR ESUR”. [54] [55]
Emerging Pediatric Research
2025 studies show lower CI-AKI rates in children (2-5%) due to resilient kidneys, but long-term NSF monitoring is advised. [56]
Impact of Saline Hydration on CI-AKI Prevention 2026 Evidence Protocols eGFR Creatinine Risk
Saline hydration is the cornerstone of 2026 CI-AKI prevention, expanding volume and diluting contrast. A 2025 Frontiers meta-analysis showed saline + oral NAC reduces CA-AKI by 22% (OR 0.78); IV NAC to OR 0.71. [11] [57] IV saline cuts risk 42% in high-risk eGFR <45. [58] [59]
Protocols: ACR 1 mL/kg/h; ESUR 1-1.5 mL/kg/h. Oral equivalent for low-risk (RR 0.97). [60] [61]
Mechanisms of Saline Hydration
Saline prevents tubular toxicity by increasing renal perfusion and urine flow, reducing contact time with contrast. [62]
Meta-Analyses Review
2025 reviews confirm superiority over no hydration, with tailored protocols (e.g., RenalGuard) yielding OR 0.32. [63] [64]
Table 4: 2026 Saline Hydration Meta-Analyses Efficacy
| Strategy | OR CI-AKI Reduction | eGFR Target | 2025/2026 Source |
|---|---|---|---|
| IV Saline | 0.58 | <45 | Meta-analysis |
| Saline + NAC | 0.47 | <30 | Frontiers |
| Tailored RenalGuard | 0.32 | <60 | NMA |
In CKD/STEMI, 58% reduction; caution in heart failure for “saline hydration impact contrast nephropathy”. [65] [66]
Subgroup Analysis
In diabetics, saline reduces risk by 35%; in pediatrics, adjusted doses prevent overhydration. [67]
Additional Risk Factors Prophylaxis 2026 Contrast Guidelines Metformin Multiple Exposures Emerging Therapies
2026 guidelines address metformin: withhold if eGFR <30. Multiple exposures: 48-hour delay for eGFR <30. Emerging SGLT2i for diabetes adjuncts; AI for eGFR risk prediction in “adjunct CI-AKI prevention”. [68] [69]
Metformin Management
Restart metformin 48 hours post-contrast if renal function stable. [70]
Contrast Volume Minimization
Keep volume <100 mL; ultra-low techniques in high-risk. [71]
Pharmacologic Adjuncts
NAC shows mixed results; statins beneficial in meta-analyses (OR 0.47). [72] [73]
Case Studies 2026 eGFR Creatinine Thresholds Saline Hydration CI-AKI Prevention
Case 1: 68-year-old diabetic, eGFR 32—ACR hydration, iso-osmolar for “safe iodinated contrast elderly CKD”. Outcome: No CI-AKI post-CT. [74]
Case 2: 3-year-old, eGFR 52—weight-based, monitor thyroid for “pediatric CI-AKI gadolinium MRI”. Outcome: Stable function. [75]
Emergency Scenarios
ER patient with unknown eGFR: Proceed with low-volume contrast if benefits outweigh risks. [76]
Challenges Future Directions Global Contrast Media Safety Low-Resource eGFR Creatinine Strategies
Low-resource: oral hydration for “cost-effective CI-AKI prevention”. Future: NGAL biomarkers, AI “contrast-induced nephropathy detection 2026”. [77] [78]
Global Disparities
In Africa/Asia, guideline adherence varies; 2026 WHO initiatives aim for standardization. [79]
Conclusion: Optimizing 2026 Contrast Safety eGFR Saline Hydration Pediatric Guidelines ACR ESUR KDIGO
2026 guidelines empower safe contrast use via eGFR-driven decisions, saline’s proven impact, and pediatric specifics, curbing CI-AKI globally. [80]
References
- American College of Radiology. (2025). ACR manual on contrast media. American College of Radiology. https://www.acr.org/Clinical-Resources/Contrast-Manual
- American College of Radiology. (2025). Statement from Drugs and Contrast Media Committee on Supervision of Contrast Material Administration. American College of Radiology. https://www.acr.org/Clinical-Resources/Clinical-Tools-and-Reference/Contrast-Manual/supervision-of-contrast-material-administration
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. (2024). KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International, 105(4S), S117-S314. https://doi.org/10.1016/j.kint.2023.10.018
- Kidney Disease: Improving Global Outcomes (KDIGO) AKI Work Group. (2012). KDIGO clinical practice guideline for acute kidney injury. Kidney International Supplements, 2(1), 1-138. https://kdigo.org/guidelines/acute-kidney-injury
- Davenport, M. S., Perazella, M. A., Yee, J., Dillman, J. R., Fine, D., McDonald, R. J., Rodby, R. A., Wang, C. L., & Weinreb, J. C. (2020). Use of intravenous iodinated contrast media in patients with kidney disease: Consensus statements from the American College of Radiology and the National Kidney Foundation. Radiology, 294(3), 660-668. https://doi.org/10.1148/radiol.2019192094
- Nijssen, E. C., Rennenberg, R. J., Nelemans, P. J., Essers, B. A., Janssen, M. M., Vermeeren, M. A., Ommen, V. V., & Wildberger, J. E. (2017). Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): A prospective, randomised, phase 3, controlled, open-label, non-inferiority trial. The Lancet, 389(10076), 1312-1322. https://doi.org/10.1016/S0140-6736(17)30057-0
- Nijssen, E. C., Rennenberg, R. J., Nelemans, P. J., Essers, B. A., Janssen, M. M., Vermeeren, M. A., Ommen, V. V., & Wildberger, J. E. (2018). Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): Long-term results of a prospective, randomised, controlled trial. EClinicalMedicine, 4-5, 48-58. https://doi.org/10.1016/j.eclinm.2018.09.006
- Timal, R. J., Kooiman, J., Sijpkens, Y. J. W., de Vries, J. P. M., Verberk-Jonkers, I. J. A. M., Brulez, H. F. H., van Buren, M., van der Molen, A. J., Cannegieter, S. C., Putter, H., van der Bom, J. G., Rabelink, T. J., Schalij, M. J., van Zwet, E. W., Huisman, M. V., & Jukema, J. W. (2020). Effect of no prehydration vs sodium bicarbonate prehydration prior to contrast-enhanced computed tomography in the prevention of postcontrast acute kidney injury in adults at high risk for contrast nephropathy: A randomized clinical trial. JAMA Network Open, 3(2), e200076. https://doi.org/10.1001/jamanetworkopen.2020.0076
- Chuah, A. M., & Yap, J. (2025). Contrast-induced acute kidney injury and nephrogenic systemic fibrosis in children: A review. Pediatric Nephrology. https://doi.org/10.1007/s00467-025-06916-w
- Francis, J. (2024). KDIGO 2024 guidelines—key points for pediatricians. JAMA Pediatrics. https://doi.org/10.1001/jamapediatrics.2024.4726
- Lin, I. C., Wu, M. T., Chen, S. B., Hwang, S. J., Tsai, W. C., & Hsu, Y. H. (2025). Saline and N-acetylcysteine-based strategies and other approaches to prevent the risk of CA-AKI: A meta-analysis. Frontiers in Medicine, 12, 1608626. https://doi.org/10.3389/fmed.2025.1608626
- Cossette, F., Standridge, S., Nagavally, S., Sell, J., & Dowling, T. (2022). Systematic review and meta-analysis of prophylaxis use with intravenous contrast exposure to prevent contrast-induced nephropathy. European Journal of Radiology, 150, 110276. https://doi.org/10.1016/j.ejrad.2022.110276
- Isaka, Y., Hayashi, H., Aonuma, K., Horio, M., Terada, Y., Doi, K., Fujigaki, Y., Yasuda, H., Sato, T., Fujikura, T., Kuwatsuru, R., Toei, H., Imai, E., & Hirayama, A. (2019). Guideline on the use of iodinated contrast media in patients with kidney disease 2018. Japanese Journal of Nephrology, 61(1), 3-46. https://pmc.ncbi.nlm.nih.gov/articles/PMC6949208
- European Society of Urogenital Radiology. (2025). ESUR guidelines on contrast agents, version 10. https://www.esur.org/esur-guidelines-2025
- Goldfarb, S., McCullough, P. A., McDermott, J., & Gay, S. B. (2009). Contrast-induced acute kidney injury: Specialty-specific protocols for interventional radiology, diagnostic computed tomography radiology, and interventional cardiology. Mayo Clinic Proceedings, 84(2), 170-179. https://doi.org/10.4065/84.2.170
- Heyman, S. N., Rosenberger, C., & Rosen, S. (2010). Acute kidney injury: Lessons from experimental models. Contributions to Nephrology, 169, 286-296. https://doi.org/10.1159/000313779
- Everson, M., Preece, J., & Woodmansey, E. (2020). Contrast-associated acute kidney injury. BJA Education, 20(11), 376-382. https://doi.org/10.1016/j.bjae.2020.06.004
- Lee, Y., Kim, S. Y., Song, Y., Kim, S. H., & Seo, J. W. (2024). Outpatient renal function screening before contrast-enhanced CT examinations. Korean Journal of Radiology, 25(10), 912-921. https://doi.org/10.3348/kjr.2024.0456
- Wang, K. C., Lee, C. H., & Chen, K. Y. (2025). Use of iodinated and gadolinium-based contrast media in patients with chronic kidney disease: Consensus statements from nephrologists, cardiologists, and radiologists. Journal of the Formosan Medical Association. https://doi.org/10.1016/j.jfma.2025.03.005
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. (2024). KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney International Supplements. https://kdigo.org/guidelines/ckd-evaluation-and-management
- Barrett, T., Fisher, R., Williams, S. P., Topping, C., Yoo, S. H., Alveyn, E., Campani Nygaard, L., McHugh, D., Kutlu, R., & Graves, M. J. (2021). Acute kidney injury: Prevention, detection, and management. Summary of updated NICE guidance for adults receiving iodine-based contrast media. Clinical Radiology, 76(3), 193-199. https://doi.org/10.1016/j.crad.2020.11.109
- Macdonald, D. B., Hurrell, C., Ferré, J. C., Maio, A., McInnes, M., Siddiqui, M., & van Rensburg, J. (2022). Canadian Association of Radiologists guidance on contrast-associated acute kidney injury. Canadian Journal of Kidney Health and Disease, 9, 20543581221097455. https://doi.org/10.1177/20543581221097455
- Li, Q., & Qin, X. (2022). Contrast-associated acute kidney injury: Advances and challenges. International Journal of General Medicine, 15, 1537-1546. https://doi.org/10.2147/IJGM.S341072
- Chinese Society of Nephrology. (2022). Expert consensus on prevention and treatment of iodine contrast media-induced acute kidney injury. Chinese Journal of Nephrology, 38(1), 1-10. https://doi.org/10.3760/cma.j.cn441217-20210909-00041
- Pelsers, M. M., Hermens, W. T., & Glatz, J. F. (2005). Fatty acid-binding proteins as plasma markers of tissue injury. Clinica Chimica Acta, 352(1-2), 15-35. https://doi.org/10.1016/j.cccn.2004.09.001
- Levin, A., & Stevens, P. E. (2024). Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: Known knowns and known unknowns. Kidney International, 105(4), 684-701. https://doi.org/10.1016/j.kint.2023.10.016
- Navaneethan, S. D., Navaneethan, S. D., & Madero, M. (2025). KDOQI US commentary on the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. American Journal of Kidney Diseases, 85(2), 135-176. https://doi.org/10.1053/j.ajkd.2024.09.977
- Awdishu, L., & Mehta, R. L. (2025). KDIGO 2024 clinical practice guideline on evaluation and management of chronic kidney disease: A primer on what pharmacists need to know. American Journal of Health-System Pharmacy, 82(12), 660-668. https://doi.org/10.1093/ajhp/zxac098
- NephJC. (2024). The KDIGO CKD 2024 guidelines part 1: Evaluation and risk stratification. http://www.nephjc.com/news/kdigo-ckd-part1
- U.S. Food and Drug Administration. (2022). FDA recommends thyroid monitoring in babies and young children who receive injections of iodine-containing contrast media for medical imaging. https://www.fda.gov/drugs/drug-safety-and-availability/fda-recommends-thyroid-monitoring-babies-and-young-children-who-receive-injections-iodine-containing
- Pediatric Endocrine Society. (2022). PES statement on thyroid monitoring in infants and young children receiving iodine-containing contrast media. https://pedsendo.org/news-announcements/pes-statement-on-thyroid-monitoring-in-infants-and-young-children-receiving-iodine-containing-contrast-media
- Wang, C. L., Schalekamp, S., Davenport, M. S., Mayo-Smith, W., & Abujudeh, H. H. (2025). Management and prevention of hypersensitivity reactions to radiocontrast media. Radiology, 315(2), e240100. https://doi.org/10.1148/radiol.240100
- Mandurino-Mirizzi, A., Munhoz, D., Crimi, G., & Leonardi, S. (2022). Contrast-associated acute kidney injury. Journal of Clinical Medicine, 11(8), 2167. https://doi.org/10.3390/jcm11082167
- van der Molen, A. J., Reimer, P., Dekkers, I. A., Bongartz, G., Bellin, M. F., Bertolotto, M., Clement, O., Heinz-Peer, G., Stacul, F., Webb, J. A. W., & Thomsen, H. S. (2025). Part 1. Management of immediate and non-immediate hypersensitivity reactions in adults. Updated guidelines by the ESUR Contrast Media Safety Committee. European Radiology. https://doi.org/10.1007/s00330-025-11675-1
- Sebastià, C., Páez-Carpio, A., Guillen Del Castillo, E., Quiroga Gómez, S., Boyé de la Tour, R., & Nicolau, C. (2020). Prophylaxis against postcontrast acute kidney injury (PC-AKI): Updates in the ESUR guidelines 10.0 and critical review. Radiología (English Edition), 62(2), 89-99. https://doi.org/10.1016/j.rxeng.2019.11.007
- Goldfarb, S., McCullough, P. A., McDermott, J., & Gay, S. B. (2009). Contrast-induced acute kidney injury: Specialty-specific protocols for interventional radiology, diagnostic computed tomography radiology, and interventional cardiology. Mayo Clinic Proceedings, 84(2), 170-179. https://doi.org/10.4065/84.2.170
- Myung, J. W., Kim, H. G., Lee, H., Kim, J. S., Park, H. J., Kim, Y. J., & Suh, C. H. (2020). Contrast-induced acute kidney injury in radiologic management of acute ischemic stroke in the emergency setting. American Journal of Neuroradiology, 41(4), 632-636. https://doi.org/10.3174/ajnr.A6472
- Waheed, S., Atta, M. G., & Bydon, A. (2021). Trials and tribulations of diagnosing and preventing contrast-induced acute kidney injury. The Journal of Thoracic and Cardiovascular Surgery, 162(1), 334-336. https://doi.org/10.1016/j.jtcvs.2020.08.067
- Society for Cardiovascular Angiography and Interventions. (2026). Quality initiatives for prevention of contrast-induced acute kidney injury. https://www.scai.org/quality-improvement-tools/qi-tips/quality-initiatives-prevention-contrast-induced-acute-kidney-0
- Davenport, M. S. (2023). Contrast-induced acute kidney injury and cardiovascular imaging: Danger or distraction? Circulation, 147(11), 862-864. https://doi.org/10.1161/CIRCULATIONAHA.122.062783
- European Society of Urogenital Radiology Contrast Media Safety Committee. (2025). B. Renal adverse reactions (post-contrast acute kidney injury, PC-AKI). https://esur-cm.org/index.php/b-renal-adverse-reactions-2
- Aoun, J., Nicolas, D., Brown, J., Semaan, E., Addam, M., El Hachem, G., Chelala, D., & Azar, H. (2019). Maximum allowable contrast dose and prevention of acute kidney injury following cardiovascular procedures. Journal of the American Heart Association, 8(5), e011279. https://doi.org/10.1161/JAHA.118.011279
- Choi, C. H., Kim, H. Y., & Park, J. Y. (2025). Navigating contrast media hypersensitivity. Radiology, 315(1), e12568759. https://pmc.ncbi.nlm.nih.gov/articles/PMC12568759
- Liu, Y., Tan, N., Zhou, Y. L., He, P. C., Yang, J., Luo, J. F., & Chen, J. Y. (2019). Effects of intravenous hydration on risk of contrast induced nephropathy and in-hospital mortality in STEMI patients undergoing primary percutaneous coronary intervention. BMC Cardiovascular Disorders, 19(1), 87. https://doi.org/10.1186/s12872-019-1054-y
- Agarwal, S. K., Mohareb, S., Patel, A., Yacoub, R., Diogenes, A., Agrawal, S., & Menon, V. (2015). Systematic oral hydration with water is similar to parenteral hydration for prevention of contrast-induced nephropathy: An updated meta-analysis of randomised clinical data. Open Heart, 2(1), e000317. https://doi.org/10.1136/openhrt-2015-000317
- Zaki, H. A., Iftikhar, H., Shokr, M., Nada, S., & Zaghloul, S. (2022). Evaluating the effectiveness of pretreatment with intravenous fluid in reducing the risk of developing contrast-induced nephropathy: A systematic review and meta-analysis. Cureus, 14(5), e24963. https://pmc.ncbi.nlm.nih.gov/articles/PMC9172963
- Walker, H., Standridge, S., Nagavally, S., Sell, J., & Dowling, T. (2022). Systematic review and meta-analysis of prophylaxis use with intravenous contrast exposure to prevent contrast-induced nephropathy. European Journal of Radiology, 150, 110276. https://doi.org/10.1016/j.ejrad.2022.110276
- Lombardi, M., Limbruno, U., Calabrò, P., Micari, A., Cortese, B., Rigattieri, S., Tarantini, G., Rubartelli, P., Varbella, F., Gardin, A., Ceravolo, R., Menozzi, A., Schembri, P., Ledda, L., Tumscitz, C., & Berti, S. (2024). Urine alkalinisation to prevent contrast-induced acute kidney injury: The prospective, randomised, controlled, open-label TEATE trial. EuroIntervention, 20(8), e504-e514. https://doi.org/10.4244/EIJ-D-23-00706
- Chen, F., Zhou, Y., Kang, Z., Li, M., Wang, Y., & Zhu, M. (2023). Different hydration methods for the prevention of contrast-induced nephropathy in patients with elective percutaneous coronary intervention: A retrospective study. BMC Cardiovascular Disorders, 23, 364. https://doi.org/10.1186/s12872-023-03358-w
- Feng, Y., Jun, M., Wang, A. Y., Liu, J., & Perkovic, V. (2025). Predicting contrast-associated acute kidney injury. JAMA Network Open, 8(3), e250107. https://doi.org/10.1001/jamanetworkopen.2025.0107
- Siew, E. D., & Matheny, M. E. (2018). Contrast-induced acute kidney injury in the PRESERVE trial: Clinical implications and future directions. Clinical Journal of the American Society of Nephrology, 13(6), 943-945. https://doi.org/10.2215/CJN.03180318
- Mandurino-Mirizzi, A., Munhoz, D., Crimi, G., & Leonardi, S. (2022). Contrast-associated acute kidney injury. Journal of Clinical Medicine, 11(8), 2167. https://doi.org/10.3390/jcm11082167
- McDonald, J. S., McDonald, R. J., Williamson, E. E., & Kallmes, D. F. (2024). Risk of acute kidney injury following IV iodinated contrast media exposure: 2023 update, from the AJR special series on contrast media. American Journal of Roentgenology, 223(1), e2330037. https://doi.org/10.2214/AJR.23.30037
- Fakhfakh, M., Zairi, I., Messaoudi, S., & Kammoun, S. (2026). New insights into contrast-associated acute kidney injury: The key role of endothelial dysfunction. Journal of Clinical Medicine. https://pmc.ncbi.nlm.nih.gov/articles/PMC12864088
- Madero, M., Levin, A., & Stevens, P. E. (2025). Evaluation and management of chronic kidney disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2024 clinical practice guideline. Annals of Internal Medicine, 178(3), 347-355. https://doi.org/10.7326/ANNALS-24-01926
- American Diabetes Association. (2026). 11. Chronic kidney disease and risk management: Standards of care in diabetes—2026. Diabetes Care, 49(Supplement 1), S246-S261. https://doi.org/10.2337/dc26-S011
- Rudnick, M. R., & Feldman, H. I. (2025). Contrast-induced acute kidney injury: The data and the debate. Consult QD. https://consultqd.clevelandclinic.org/contrast-induced-acute-kidney-injury-the-data-and-the-debate
- UpToDate. (2026). Prevention of contrast-induced acute kidney injury associated with computed tomography. https://www.uptodate.com/contents/prevention-of-contrast-induced-acute-kidney-injury-associated-with-computed-tomography
- American College of Cardiology. (2016). Contrast-induced acute kidney injury. https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2016/09/19/15/11/contrast-induced-acute-kidney-injury
- Benghazi Dialysis Forum. (2026). New 2026 CI-AKI guide. https://www.facebook.com/100082298119905/posts/-new-2026-ci-aki-guide-benghazi-dialysis-forum-updated-recommendations-on-contra/883957747690821
- Giacoppo, D., Gargiulo, G., Buccheri, S., Aruta, P., Byrne, R. A., Cassese, S., Katagiri, Y., Laudani, C., Leonardi, S., & Mehran, R. (2017). Preventive strategies for contrast-induced acute kidney injury in patients undergoing percutaneous coronary procedures: Evidence from a hierarchical Bayesian network meta-analysis of 124 trials and 28,240 patients. Circulation: Cardiovascular Interventions, 10(5), e004383. https://doi.org/10.1161/CIRCINTERVENTIONS.116.004383
- Liu, Y., Tan, N., Zhou, Y. L., He, P. C., Yang, J., Luo, J. F., & Chen, J. Y. (2023). Simplified rapid hydration prevents contrast-associated acute kidney injury among CKD patients undergoing coronary angiography. JACC: Cardiovascular Interventions, 16(9), 1072-1084. https://doi.org/10.1016/j.jcin.2023.03.025
- Heyman, S. N., Rosenberger, C., & Rosen, S. (2025). It is not only fluids: The impact of hydration protocols used for the prevention of contrast nephropathy on renal oxygenation. Renal Failure, 47(1), 2528889. https://doi.org/10.1080/0886022X.2025.2528889
- El Gharib, K., & El Gharib, M. (2025). Effect of resuscitation with normal saline versus lactate ringer on major kidney events in patients presenting with sepsis: A systematic review and meta-analysis. American Journal of Respiratory and Critical Care Medicine, 211. https://doi.org/10.1164/ajrccm.2025.211.Abstracts.A3790
- Lin, I. C., Wu, M. T., Chen, S. B., Hwang, S. J., Tsai, W. C., & Hsu, Y. H. (2025). Saline and N-acetylcysteine-based strategies and other approaches to prevent the risk of CA-AKI: A meta-analysis. Frontiers in Medicine, 12, 1608626. https://pmc.ncbi.nlm.nih.gov/articles/PMC12647111
- American College of Radiology. (2020). ACR manual on contrast media. University of Florida. https://xray.ufl.edu/wordpress/files/2020/05/2020_ACR_Manual_Contrast_Media.pdf
- Thomsen, H. S., Morcos, S. K., Almén, T., Bellin, M. F., Bertolotto, M., Bongartz, G., Clement, O., Leander, P., Heinz-Peer, G., Reimer, P., Stacul, F., van der Molen, A., Webb, J. A. W., & ESUR Contrast Medium Safety Committee. (2011). Contrast-induced nephropathy: Updated ESUR Contrast Media Safety Committee guidelines. European Radiology, 21(12), 2527-2541. https://doi.org/10.1007/s00330-011-2225-0
- Society of Thoracic Surgeons. (2021). Trials and tribulations of diagnosing and preventing contrast-induced acute kidney injury. The Journal of Thoracic and Cardiovascular Surgery, 162(1), 334-336. https://doi.org/10.1016/j.jtcvs.2020.08.067
- EB Medicine. (2021). IV contrast and kidney injury. https://foamed.ebmedicine.net/rapid-reference/iv-contrast-and-kidney-injury
- Davenport, M. S., Cohan, R. H., & Ellis, J. H. (2015). Contrast media controversies in 2015: CT versus MRI versus nothing. Journal of the American College of Radiology, 12(11), 1184-1188. https://doi.org/10.1016/j.jacr.2015.07.026
- American College of Radiology. (2025). Contrast manual. https://cs.acr.org/Clinical-Resources/Contrast-Manual
- Ganigara, M., Eapen, R. S., & Gnanam, D. (2025). Optimizing contrast administration in pediatric cardiovascular CT: Safety and technique. Journal of Cardiovascular Computed Tomography. https://doi.org/10.1016/j.jcct.2025.04.436
- U.S. Food and Drug Administration. (2023). FDA drug safety communication: FDA recommends thyroid monitoring in babies and young children who receive injections of iodine-containing contrast media for medical imaging. https://www.fda.gov/drugs/drug-safety-and-availability/fda-recommends-thyroid-monitoring-babies-and-young-children-who-receive-injections-iodine-containing
- Yale School of Medicine. (2025). Pre-medication policy. https://medicine.yale.edu/radiology-biomedical-imaging/quality-safety/premedication
- UCSF Radiology. (2025). CT and X-ray contrast guidelines. https://radiology.ucsf.edu/patient-care/patient-safety/ct-and-x-ray-contrast-guidelines
- ContrastConnect. (2026). Pediatric CT IV contrast guidelines: Dosage & protocols. https://www.contrast-connect.com/blog-post/pediatric-ct-iv-contrast-guidelines-dosage-protocols
- Society for Pediatric Radiology. (2022). SPR endorses an ACR statement. https://www.spr.org/news/spr-endorses-an-acr-statement
- McDonald, J. S., McDonald, R. J., Williamson, E. E., & Kallmes, D. F. (2023). Risk of acute kidney injury following IV iodinated contrast media exposure: 2023 update. American Journal of Roentgenology. https://doi.org/10.2214/AJR.23.30037
- Chen, S. Y., Li, Q., & Qin, X. (2022). Contrast-associated acute kidney injury: Advances and challenges. International Journal of General Medicine, 15, 1537-1546. https://doi.org/10.2147/IJGM.S341072
- Levin, A., & Stevens, P. E. (2024). Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements. https://www.sciencedirect.com/science/article/pii/S0085253823007640